"We Care, Because Your Life Matters..."
"We Care, Because Your Life Matters..."



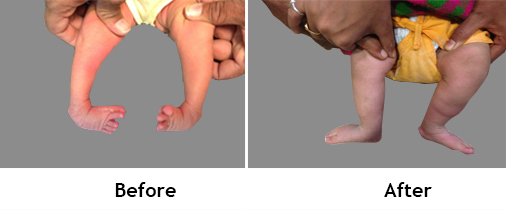
Club Foot Treatment is common congenital foot deformity Unilateral or bilateral (one side or both sides).
Incidence: One or two per 1000 live births.
We have to start treatment early from second day of life.
It will correct by serial casting (every week), 4-5 plasters by Ponseti method.
It give painless, plantigrade, and flexible foot.
I have treated more than 2000 (two thousand) by plaster.
Late presentation may require surgery.

Congenital Knee Dislocation (CDK):
It is rare deformity that present at birth as recurvatum.
Incidence: One in 100000 live births. It may associate with hip dislocation.
It can occur with myelodysplasia, Larsen syndrome, Arthrogryposis.
It may be hyperextension, subluxation or dislocation.
Treatment: Serial plaster cast.. if not corrected then require surgery.
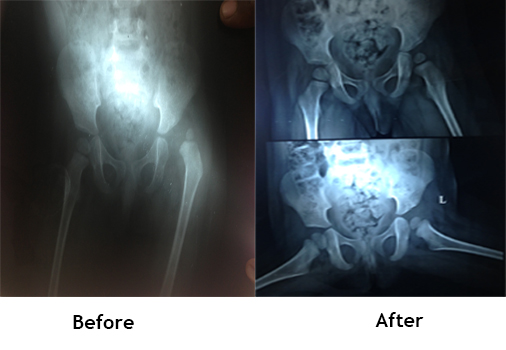
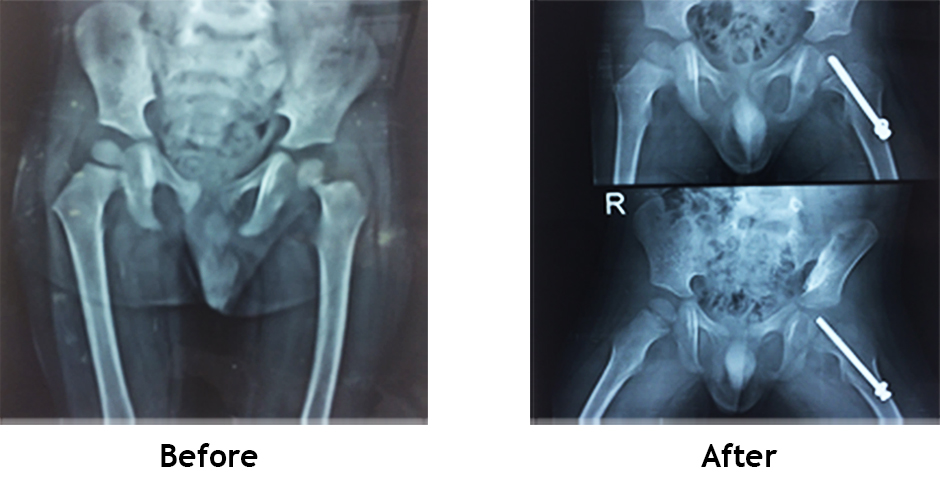
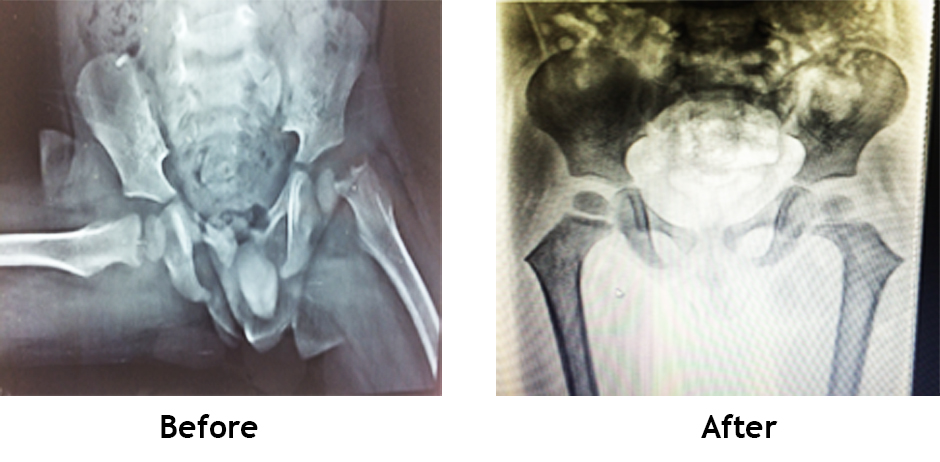
Developmental dysplasia or Hip Dislocation Treatment is disorder that may affect development and stability of hip joint during critical period of growth, either in utero or after birth.
Incidence: One in 1000 live births (unilateral or bilateral).
Diagnosis: In neonates : clicking sound during abduction / adduction of hip, Abnormal thigh fold, shortening (one side) USG in confirmative up to 4-6 months then x ray.
Walking child: Abnormal gait, painless limp.
Treatment: 0 - 3 months Pavlik harness, 3 - 6 months : Hip spica cast, 6 months – 2 year : Close reduction / open reduction plus hip spica, 2 years onward : Surgery.

Genu valgum (knock knee) both knee are going in and leg going out side Walking difficulty.
It is idiopathic, post traumatic, Rickets, skeletal dysplasia, tumors or hereditary multiple exsotoses (HME).
Genu varum (bow legs): Physiological, Blount’s disease, skeletal dysplasia, rickets, post infective or traumatic, focal fibrocartilaginous dysplasia.
Diagnosis: Clinical obvious deformity at knee X ray full length (scanogram).
Treatment: Nutritional rickets will correct deformity by medicine.
Surgery: Growth modulation by plate or staple or screw in skeletally immature patients.
Corrective osteotomy may require for skeletally mature patients.
Infection of musculoskeletal system include, osteomyelitis (bone infection), septic arthritis (Joint infection) and pyomyositis (muscles infection).
Various organism responsible for infection like staphylococcus aureus (90%), streptococcus, Haemophilus influenza, pneumococcus, klebsiella, e.coli, pseudomonas etc..
It happens due to Hematogenous spread from bacteremia, local invasion from contiguous infection, direct penetrating trauma.
Septic arthritis is 70% in children age 1 month to 5 years.
Sites: Hip (41%), Knee(23%), Ankle (14%), Elbow(12%), wrist and shoulder (4%).
Physical finding: Fever, inability to move affected limb, irritable, lethargic.
Blood report: CBC TC increased, CRP raised, ESR, blood culture.
X –ray, USG, MRI may require.
Treatment: Acute OM may be treat by injectable and oral antibiotics, chronic OM require and septic arthritis require prompt drainage or scrapping, reaming, some time antibiotic cemented bids insertion.
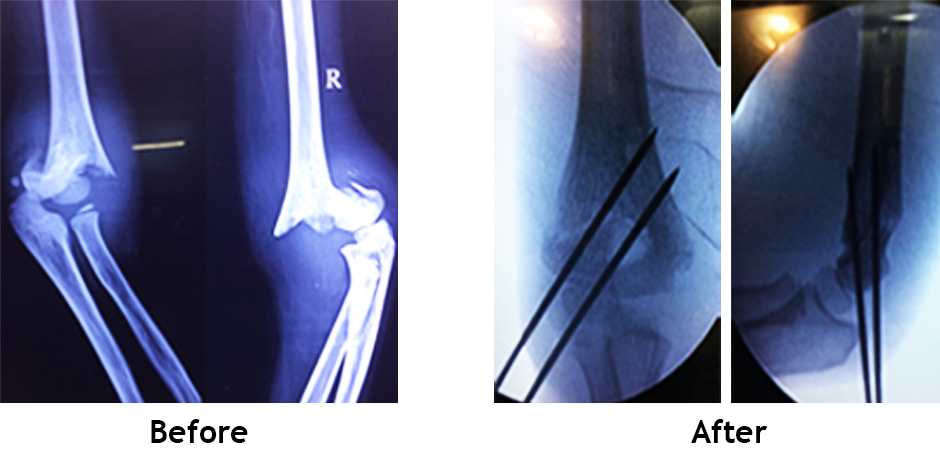
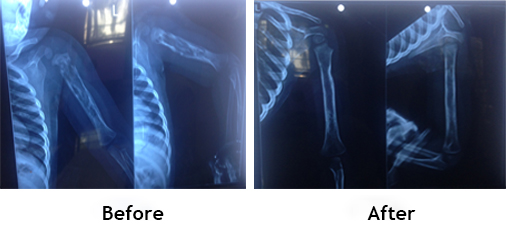
Skeletal trauma accounts for 10% to 15% of all childhood injuries. Fractures of the immature skeleton differ from those of the mature skeleton. Physeal disruptions make up about 15% of all skeletal injuries in children,Damage involving specific growth regions, such as the physis or epiphyseal ossification center, may lead to acute or chronic growth disturbance supper-extremity fractures account for 65% to 75% of all fractures in children. The most common area of the upper extremity injured is the distal forearm 7% to 9% of upper-extremity fractures involve the elbow. The distal humerus accounts for approximately 86% of fractures about the elbow region. Supracondylar fractures are the most frequent elbow injuries in children, reported to occur in 55% to 75% of patients with elbow fractures. Lateral condylar fractures are the second most common, followed by medial epicondylar fractures. Fractures of the olecranon, radial head. Forearm fractures in children are the most common long bone fractures, comprising about 40% of all pediatric fractures. Femoral shaft fractures, including subtrochanteric and supracondylar fractures, represent approximately 1.6% of all bony injuries in children.
Management : X ray affected part, comparative view, CT scan, MRI for understand physis or intraarticular fragment status.
Healing and remodeling potential is very high so most of fracture in children are treated by plaster and adolescent require surgery.